

Integrative Diagnostic Model
Our clinicians use Dr. Bastian’s unique three-step diagnostic model:
- Patient history, the story of the problem.
- The vocal capability battery, a special kind of listening to the voice to understand its capabilities, limitations, and aberrations.
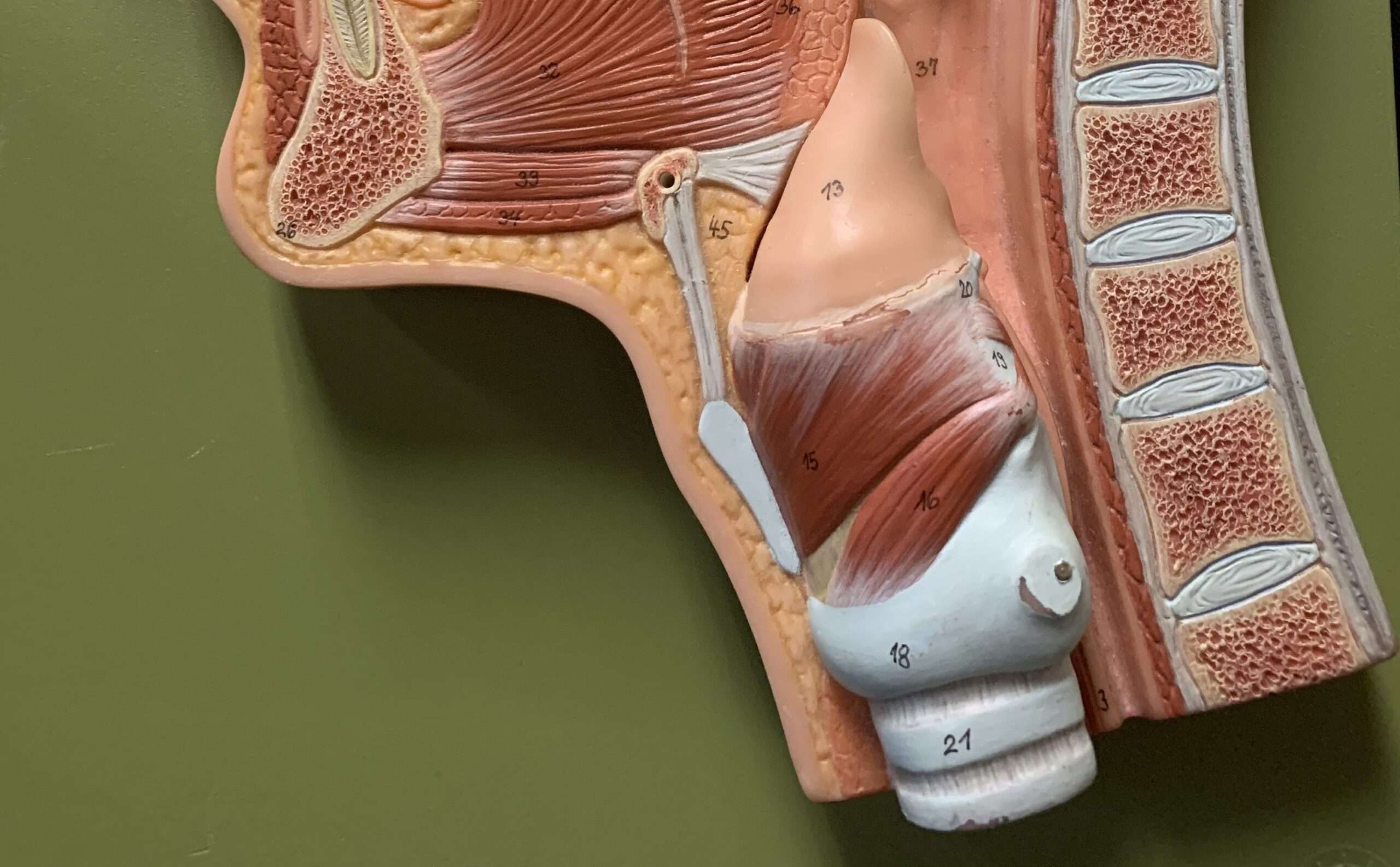
- Videoendoscopy or videostroboscopy, to examine visually the structure and function of the larynx and other parts of the upper aerodigestive tract.
Taken together, these three diagnostic components help our physicians offer a precise diagnosis on the spot.
Videostroboscopy
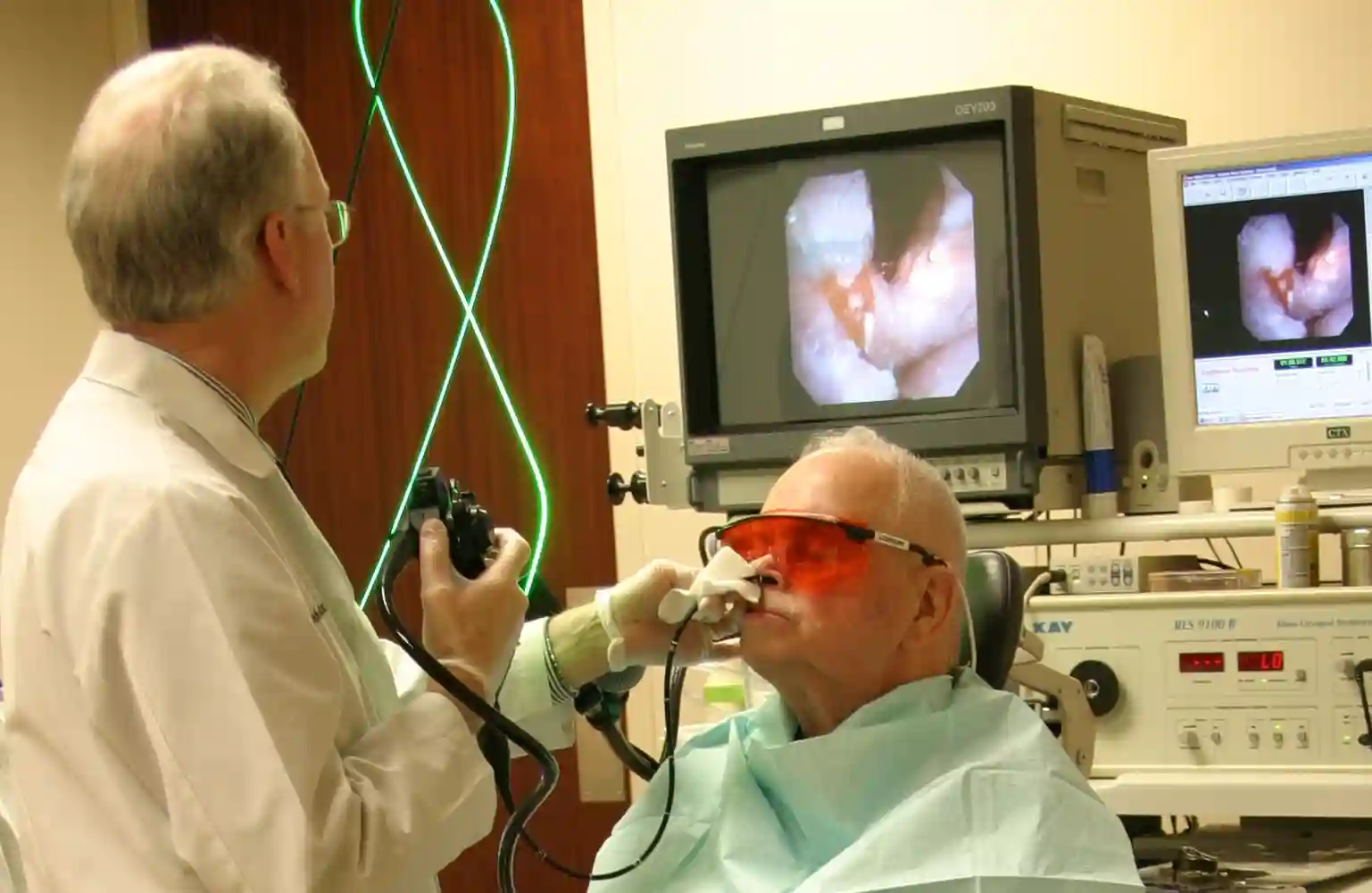
After taking the patient’s history and assessing the voice’s capabilities and limitations, BVI clinicians visually inspect the larynx, including vocal fold vibration, and other parts of the upper aerodigestive tract using state-of-the-art equipment with remarkable optical resolution and magnification. This level of visual clarity helps BVI clinicians to avoid being misled by “red herrings”—obvious but irrelevant visual findings—and also to discover more subtle visual clues.

Office-Based Surgery
Most larynx and pharynx surgeries worldwide are performed in the operating room, due to the need for general anesthesia. With the arrival of advanced digital optics and the use of topical (local) anesthesia, however, Drs. Bastian and Richardson handle many such procedures in a specially equipped videoendoscopy room (with pulsed-KTP and Thulium fiberoptic lasers) in the office—saving patients both time and money.
Vocal Fold Microsurgery
Many people—especially professional singers—may suffer from hoarseness or other vocal problems caused by vibratory damage, or by other lesions on their vocal folds. Drs. Bastian, Richardson and Hoesli have particular expertise and experience in surgically treating injuries that otherwise will not resolve. They have operated on an estimated 1,500 singers, as well as thousands of non-singer patients.
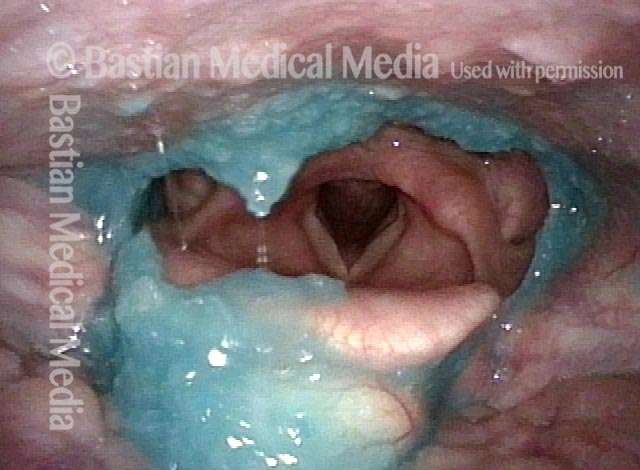
Videoendoscopic Swallowing Study (VESS)
Developed by Dr. Bastian as a way to evaluate swallowing problems. The clinician uses a flexible endoscope positioned just above the patient’s palate to watch from inside as the patient swallows blue-colored applesauce, or water, or orange-colored cheese crackers. The x-ray-based videofluoroscopic swallowing study (VFSS) is also performed at a nearby facility, when needed.
Surgery for Antegrade Cricopharyngeus Muscle Dysfunction (A-CPD)
This disorder causes people to have progressive difficulty in swallowing, particularly solid foods and pills: the cricopharyngeus muscle fails to relax and allow material to pass through. To treat this disorder—with or without a Zenker’s diverticulum, a herniated pouch that collects food and saliva—BVI clinicians have been in the vanguard of physicians using endoscopic (through-the-mouth) laser surgery, in preference to the more traditional neck-incision approach.

Larynx Cancer Surgery
Methods for treating larynx cancer include surgery, radiation, and chemotherapy. For smaller tumors in particular, laser excision through the mouth can offer dramatic advantages. BVI clinicians have a large and noteworthy experience with larynx cancer, including not only endoscopic laser approaches but also (when tumors are very advanced) partial or total laryngectomy.
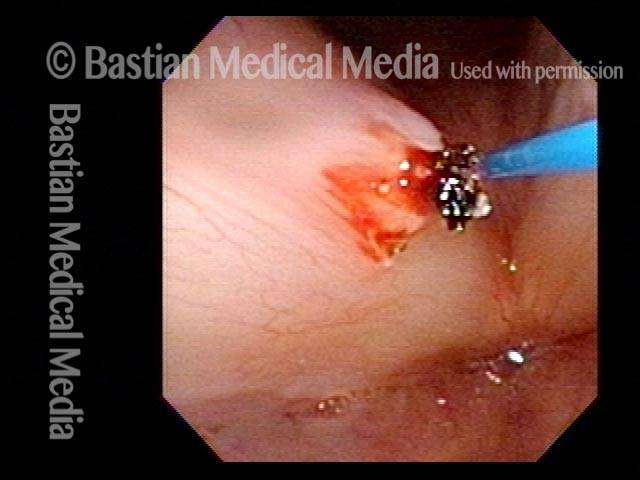
Biopsy of selected lesions of the larynx, pharynx, trachea, or esophagus
At BVI, the majority of biopsies are performed on-site, in the videoendoscopy procedure room. A return to this approach was pioneered by Dr. Bastian. On-site BVI biopsies are performed using special endoscopes and other instruments along with video apparatus. The individual is topically anesthetized and sometimes mildly sedated. If unsedated, the individual can drive himself or her-self to and from the procedure. BVI physicians continue to use “traditional” operating room biopsy techniques in situations where that approach is better suited.
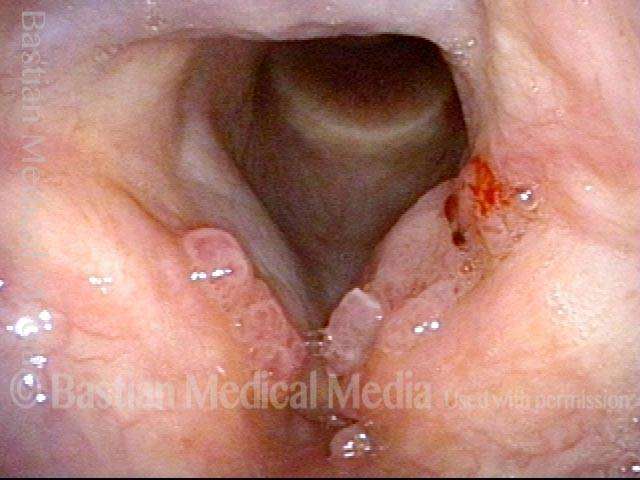
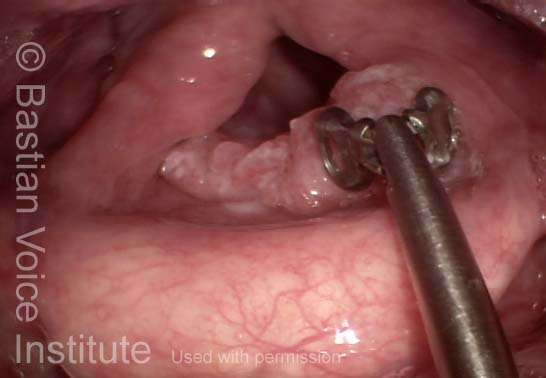
Treatment for Recurrent Respiratory Papillomatosis (RRP)
RRP is caused by chronic infection with the human papillomavirus (HPV). The result is a proliferation of wart-like lesions within the larynx and, occasionally, the trachea. BVI has a caseload of 170 adult patients. Our clinicians have been quick to test or adopt adjuvants (supporting treatments to surgery) such as interferon, indole-3-carbinol, cidofovir, artemisinin, and avastin.
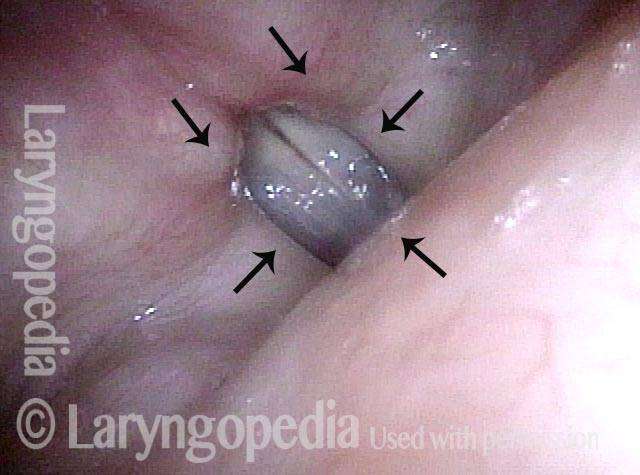
Botox™ Injections for Spasmodic Dysphonia (SD)
SD is a rare neurological disorder which affects voice control. The most effective treatment in widespread use is periodic injection of Botox™ into the muscles of the larynx. Typically, three or four injections per year are sufficient to keep the voice functioning at a much improved level. BVI clinicians were among the first in the country to use Botox™ for treating SD, dating back to 1989. They currently perform about 80 Botox™ injections per month,

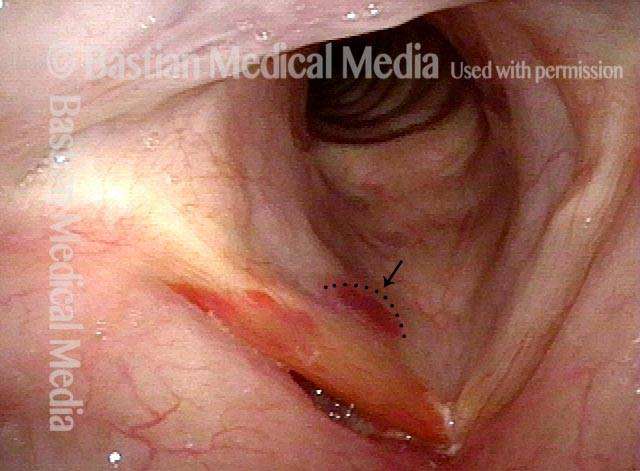
Vocal Fold Injections or Implants for Paralysis
For people suffering from a weak, breathy voice caused by vocal fold paralysis or atrophy, BVI offers voice gel injections (for temporary benefit, though typically lasting many months). When the neurological impairment is known to be permanent, then silastic or other implant material may be inserted into the fold through a neck incision, with the patient under local anesthesia with sedation in an outpatient setting.
Sensory Neuropathic Cough Treatment (SNC)
More than 15 years ago, Dr. Bastian discovered a neurogenic form of coughing, which he terms “sensory neuropathic cough.” Management includes titration trials of various neuralgia medications. BVI has since attracted as many as 1,000 such patients from as far away as Brazil. Many of these patients are managed over time from great distance, via phone follow-up.
Retrograde Cricopharyngeus Dysfunction (R-CPD) | Inability to Burp
Another BVI discovery is a previously unknown disorder causing severe daily distress of inability to belch, socially-awkward gurgling noises, bloating and other abdominal distress and in most cases excessive flatulence. A single injection of Botox into the upper esophageal sphincter resovles this problem permantly in 4 of 5 patients. So far (January 2024) BVI doctors have treated over 1,600 patients from all 50 states and 25 foreign countries.