Vocal Fold Injuries
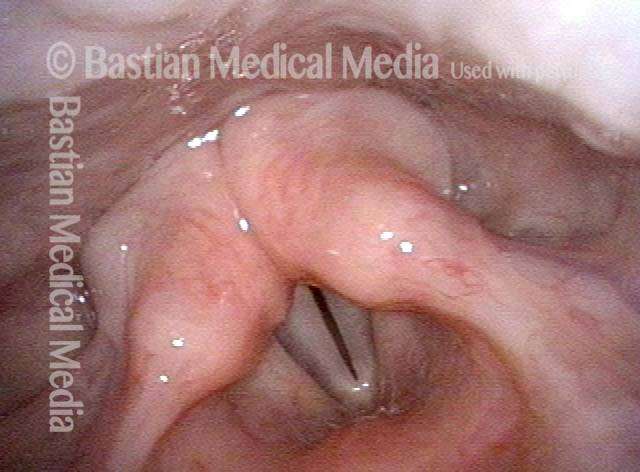
Lesions (abnormal tissue) on the surface tissue of the vocal folds, typically caused by vocal overuse. These include:
- Nodules (pictured)
- Polyps
- Capillary ectasia
- Epidermoid cysts
- Glottic sulcus
- Smoker’s polyps

Other Benign Lesions and Conditions of the Larynx
Lesions or conditions that arise in the larynx but, unlike vocal fold injuries, usually without correlation to voice use. These include:
- Contact or intubation granulomas
- Mucus retention cysts (pictured)
- Saccular cysts
- Laryngopharynx acid reflux
- Laryngitis
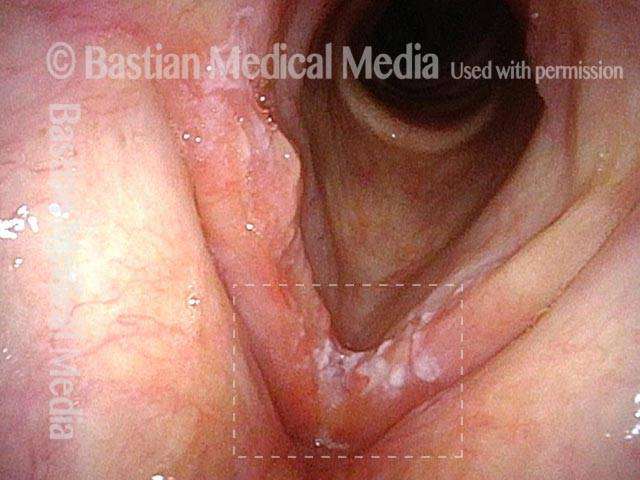
Cancer of the Larynx and Pharynx
A malignant growth or tumor caused by abnormal, uncontrolled cell division. Local tumors are described as one of the following:
- T1, earliest and smallest (pictured)
- T2
- T3
- T4

Recurrent Respiratory Papillomatosis (RRP)
Wart-like lesions in the larynx or trachea, caused by chronic infection with HPV (human papillomavirus).
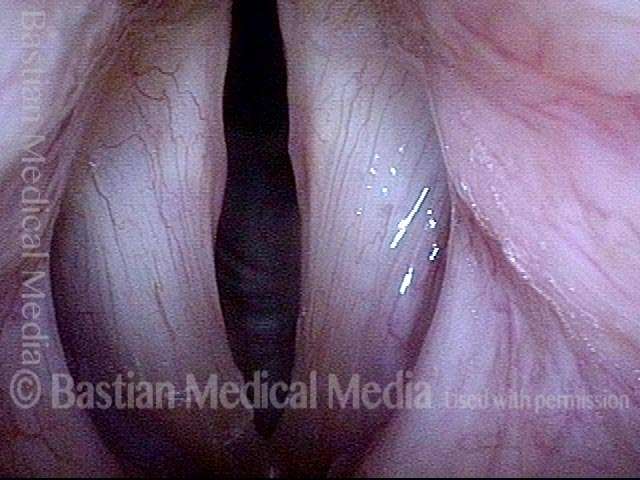
Spasmodic dysphonia (SD)
Neurological disorder in which muscles of the larynx spasm, either choking off or straining the voice or else making it breathy or drop abruptly to a whisper mid-word or sentence:
- Adductory (AD): chokes off or strains
- Abductory (AB): breathy or whispery (pictured)
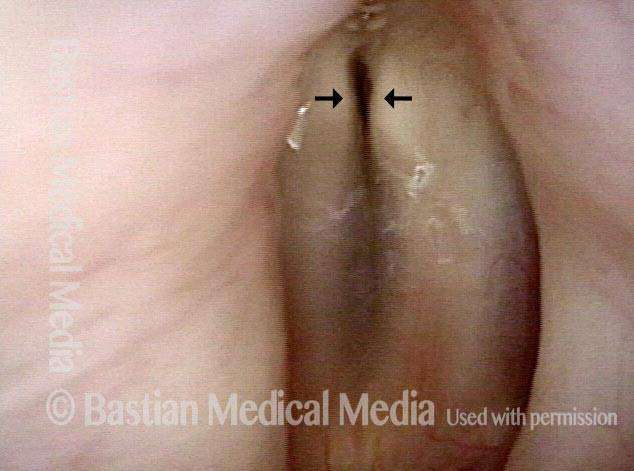
Vocal fold paralysis
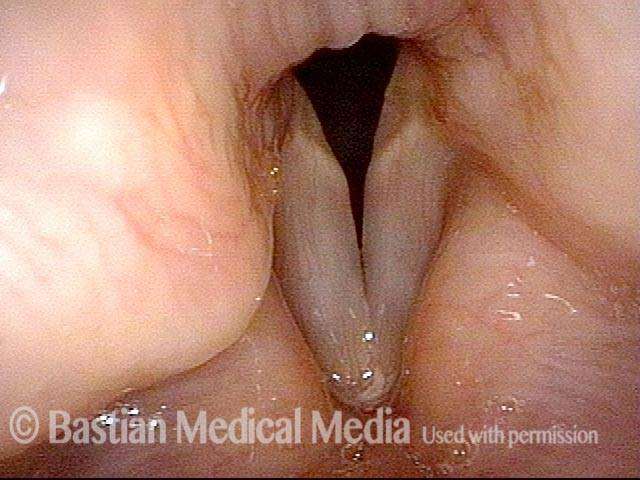
Neurological disorder in which one or both vocal folds are paralyzed, causing a weak, breathy voice or difficulty breathing, respectively. Variants include:
- Unilateral paralysis (pictured)
- Bilateral paralysis
- Paresis (weakness, or partial paralysis)
Professional voice disorders
More often than not, the difficulties encountered by professional voice users resolve or diminish to an acceptable level through a combination of medical, speech therapy, and “life strategy” maneuvers. Vocal fold microsurgery (above) is an option for irreversible lesions.

Swallowing Dysfunction
We focus on mouth and throat-related swallowing difficulties, from poor muscular propulsion of food material or from failure of other muscles to relax and let food material pass through:
- Presbyphagia (propulsion)
- Cricopharyngeus dysfunction (non-relaxation), with/without Zenker’s diverticulum (pictured)
Airway Stenosis
Stenosis (narrowing) of the airway at the vocal folds, just below them, or down into the trachea can lead to noisy breathing, reduced exercise tolerance, etc. Causes may include:
- Scarring: post-intubation injury
- Scarring: prior tracheotomy
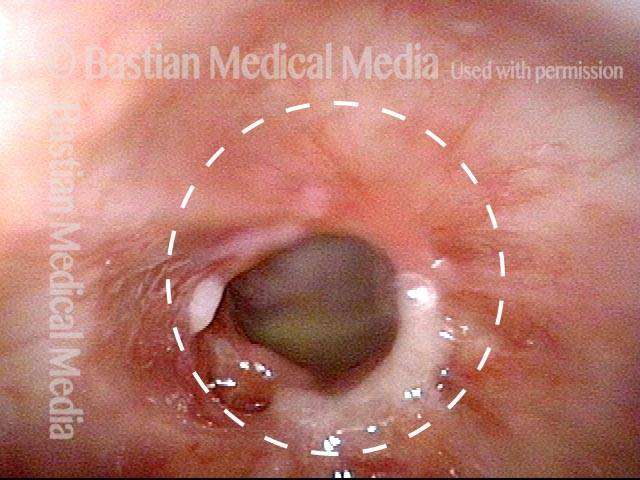
- Inflammation: Wegener’s granulomatosis (pictured)

Sensory Neuropathic Cough
Variant of chronic cough discovered by Dr. Bastian years ago. A neurogenic cough, often mistakenly thought to be the result of asthma, acid reflux, allergy, or stress/psychological factors.
Non-Organic Disorders
Disorders that arise not from dysfunction of the mechanism itself but instead from how the mechanism is used. These disorders can affect:
- Voice
- Breathing (pictured)
- Coughing