Zenker’s Diverticulum (ZD) is an outpouching or, in effect, a hernia of the swallowing passage just above a non-relaxing cricopharyngeus muscle.
In essence, the forces of swallowing are delivered against a somewhat unyielding muscle, and this causes the wall of the swallowing passage just above the cricopharyngeus muscle (i.e., the upper esophageal sphincter) to balloon outward. Hence, unknown to many, the Zenker’s diverticulum is only the reflection of the main problem, which is cricopharyngeal dysfunction.
Treatment for ZD
Myotomy of the cricopharyngeus muscle tends to resolve symptoms, even though the Zenker’s diverticulum is left in place and not removed.
Photo Essays of Zenkers Diverticulum
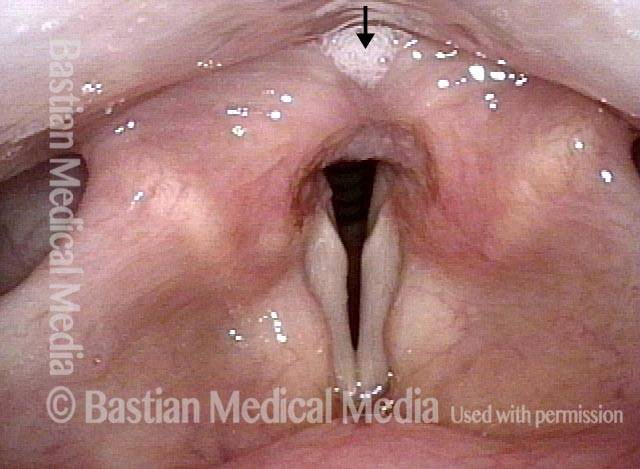
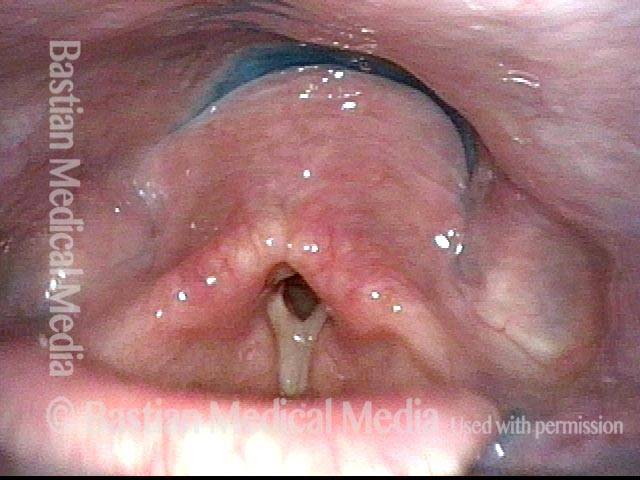
Zenker’s diverticulum (1 of 4)

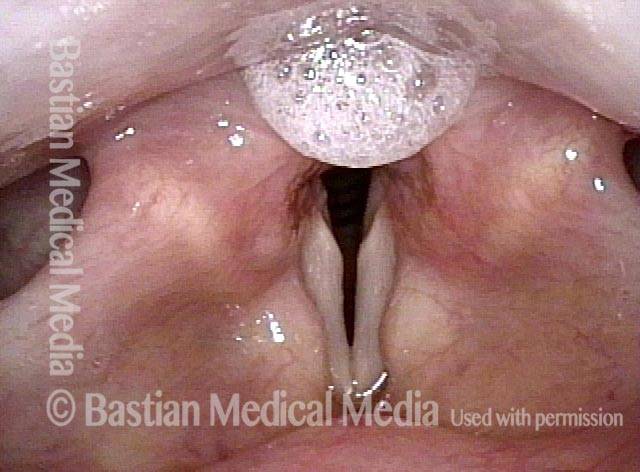
Saliva from Zenker’s sac (2 of 4)
More saliva (3 of 4)
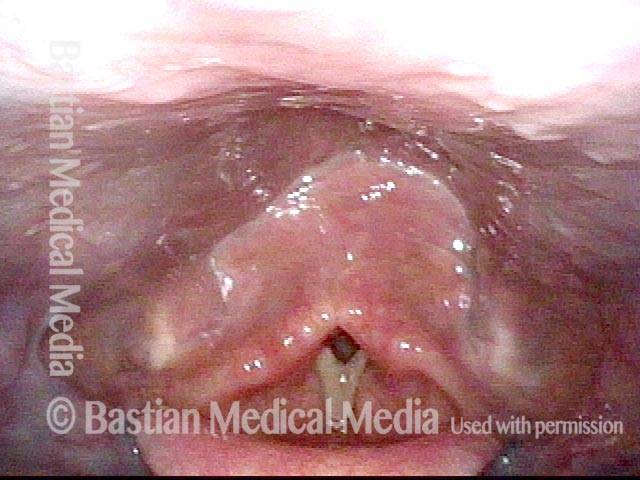
Forced to re-swallow (4 of 4)

Example 2
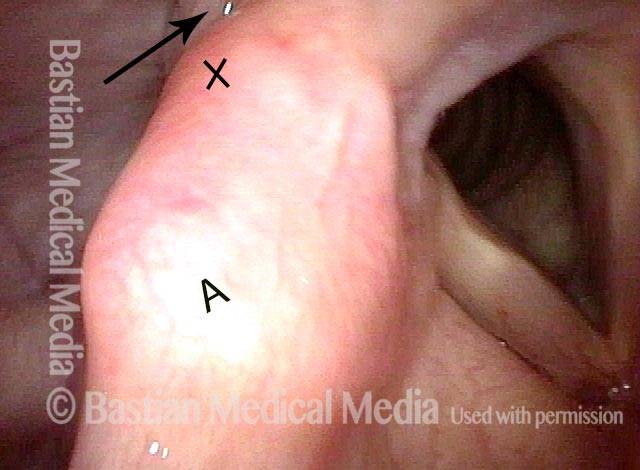
Zenker’s diverticulum (1 of 3)

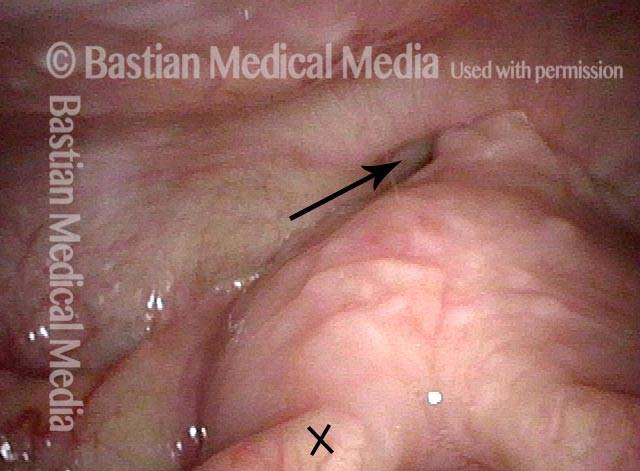
Postcricoid area (2 of 3)

Hypopharynx (3 of 3)

Post-swallow Return of Saliva into the Hypopharynx
This man began to experience solid food lodgment a few years earlier, along with gurgling noises every time he swallows. Even on an initial examination, Zenker’s diverticulum can be strongly suspected based on the findings of the videoendoscopic swallow study (VESS). Upon review of a videofluoroscopic swallow study (VFSS), a Zenker’s diverticulum is indeed the explanation for the findings below, which went away completely (return of saliva, gurgling noises, and food lodgment) after myotomy.
Pooling of saliva (1 of 4)

Saliva disappears after swallow (2 of 2)

Saliva begins to return (3 of 3)

Saliva is ejected upwards from Zenker’s sac (4 of 4)

Reflux Into Hypopharynx, Characteristic of Cricopharyngeal Dysfunction
Reflux into hypopharynx (1 of 3)
Water flows into the swallowing crescent (2 of 3)
Larynx opens up (3 of 3)

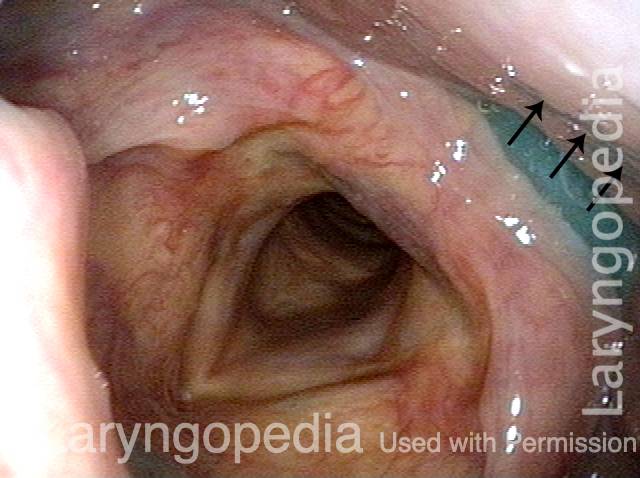
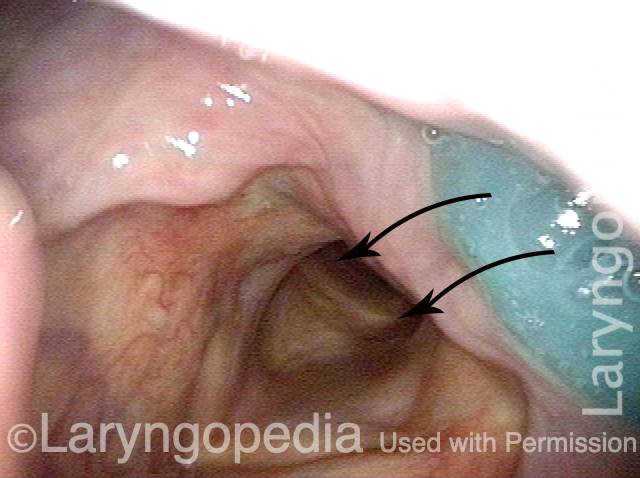
Videoendoscopic View of Zenker’s Sac Opening and Cricopharyngeus Bar
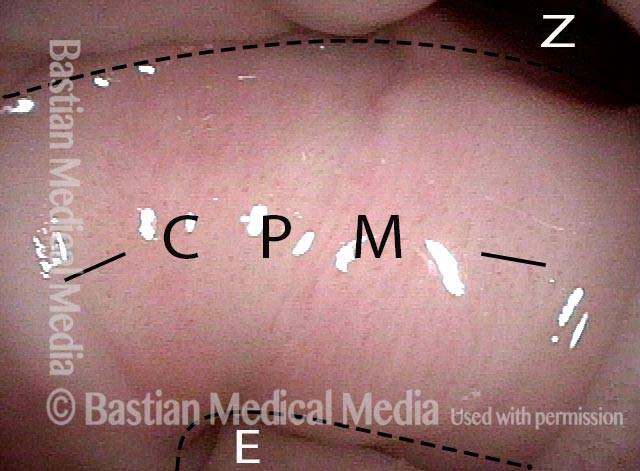
Orientation (1 of 4)
View into post-arytenoid and post-cricoid area (2 of 4)
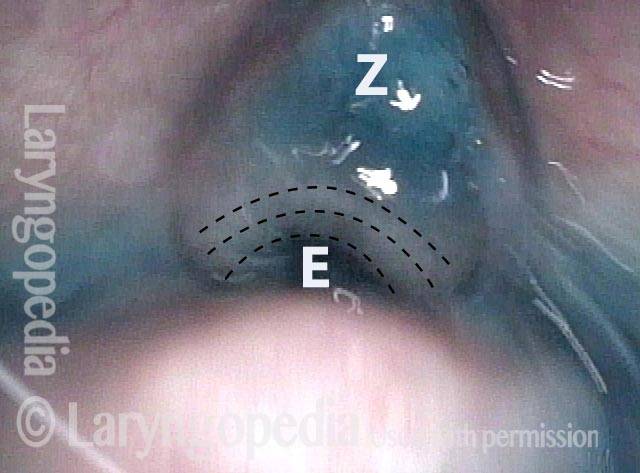
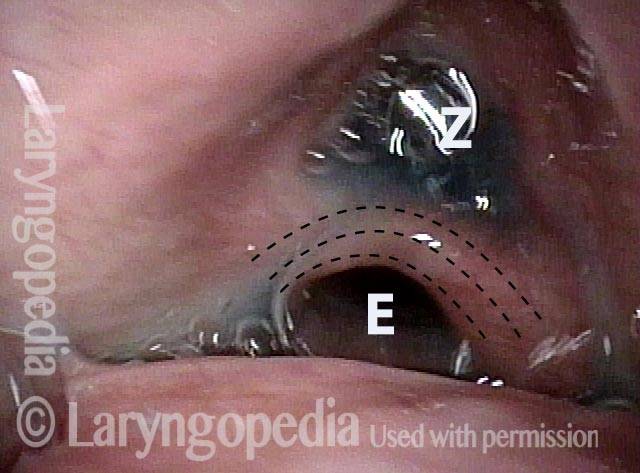
Esophageal and Zenker sac openings (3 of 4)
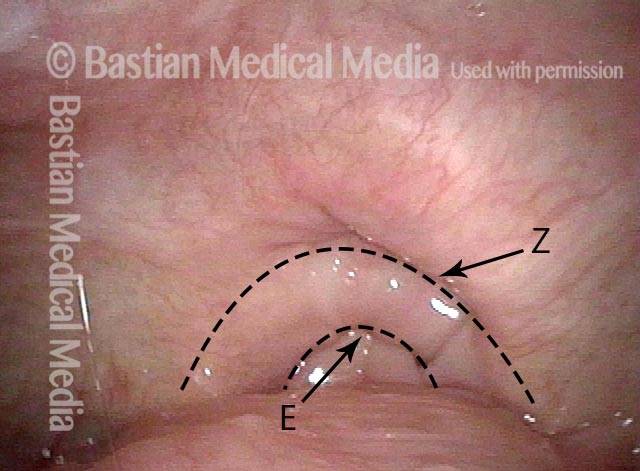
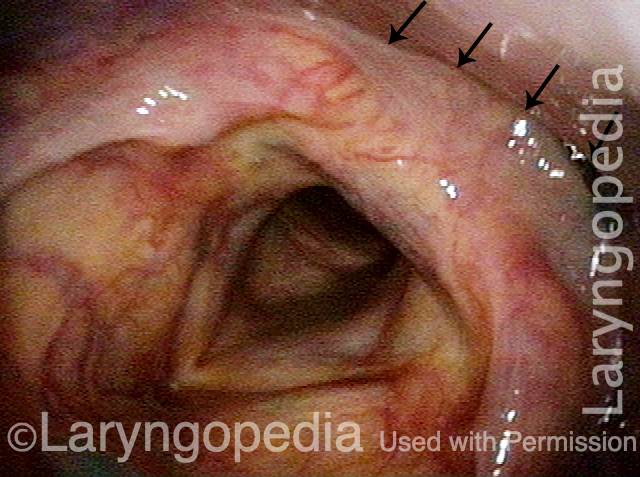
Cricopharyngeus muscle bar (4 of 4)
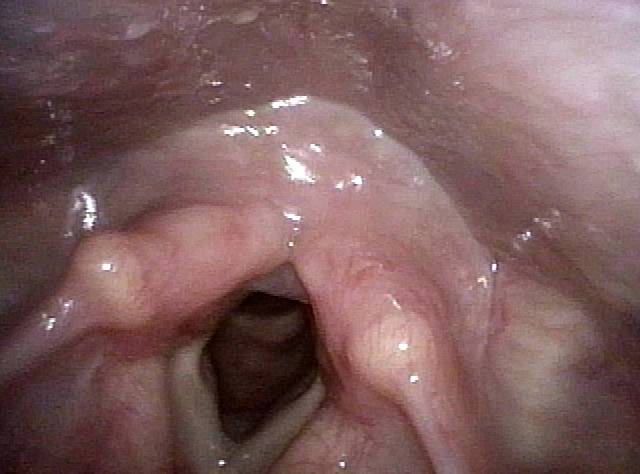
Cricopharyngeus Non-Relaxation and Zenker’s Sac Seen During VESS
Immediately after swallow (1 of 4)

One second later (2 of 4

Un-relaxed cricopharyngeus muscle (3 of 4)
More water (4 of 4)
Zenker’s Diverticulum Returns Its Contents Upwards to the Throat After Each Swallow
VESS (1 of 3)
Swallowing Crescent (2 of 3)
Applesauce spills into airway (3 of 3)
Post-swallow Hypopharyngeal Reflux (Zenker’s Diverticulum): VESS vs. VFSS
VESS (1 of 7)

Reflux (2 of 7)

Post-swallow (3 of 7)
Reflux of cracker (4 of 7)

VFSS (5 of 7)

X-Ray (6 of 7)

Continued reflux (7 of 7)

{kind=link}