Subtype 6
More common subtype seen in the airway. HPV 6 is associated with a lesser risk of cancer formation, as is HPV 11.
Humility Before the HPV Virus—A Recurrence of Papillomas at Ten Years
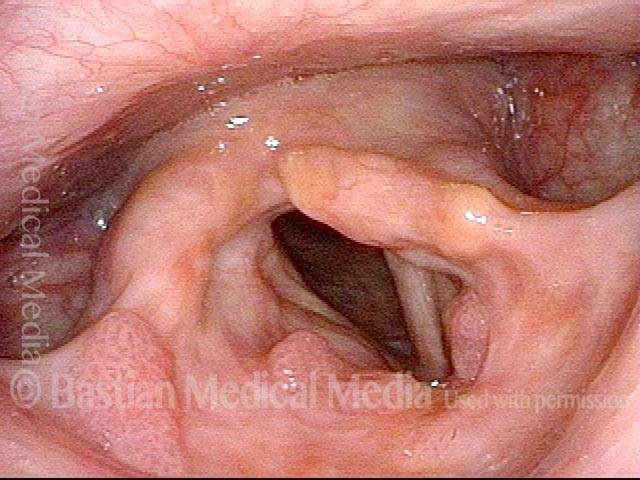
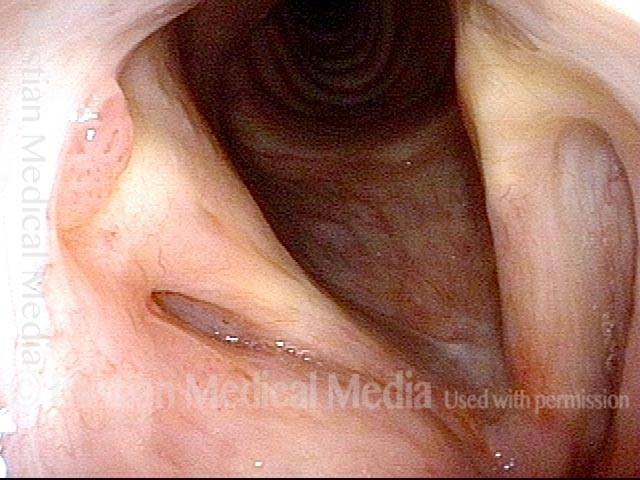
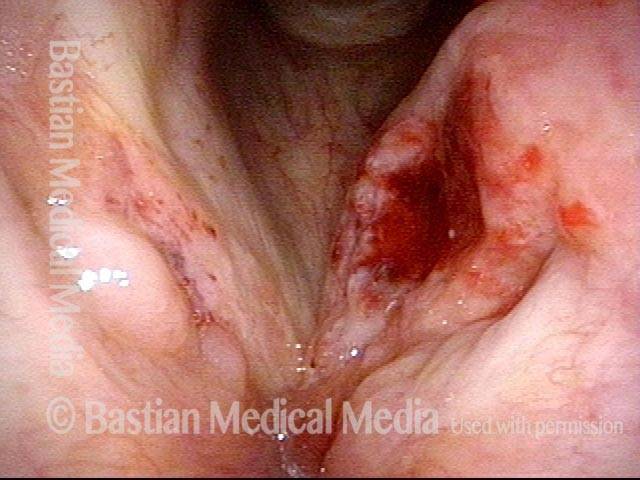
HPV infection is considered chronic, and causes recurrent growth of papillomas in the larynx. Still, we sometimes see what appear to be cures, or at least long-term remissions. That appears to be the case here. After an 8 year interval of perfect voice, the patient had a sudden increase of hoarseness occurring in the few weeks prior to the last examination below.
This is an illustration of why we often say to a patient who appears to be cured, “You may be cured, but we usually say “long term remission.” This patient’s scenario is not rare. Was her longterm, 8-year remission due to meticulous surgery? Cidofovir? Her immune response? It is impossible to say if it was one or all of these factors.
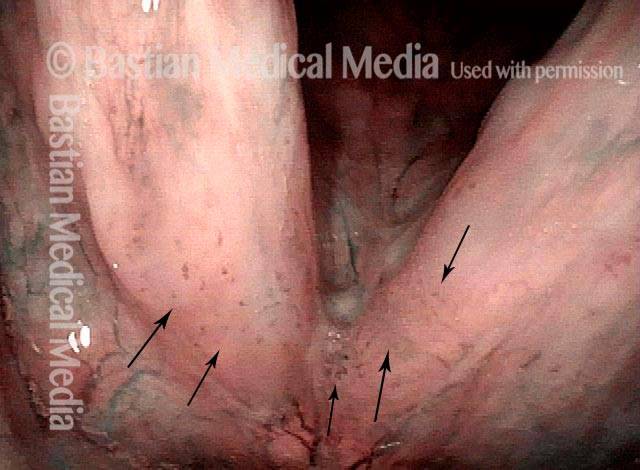
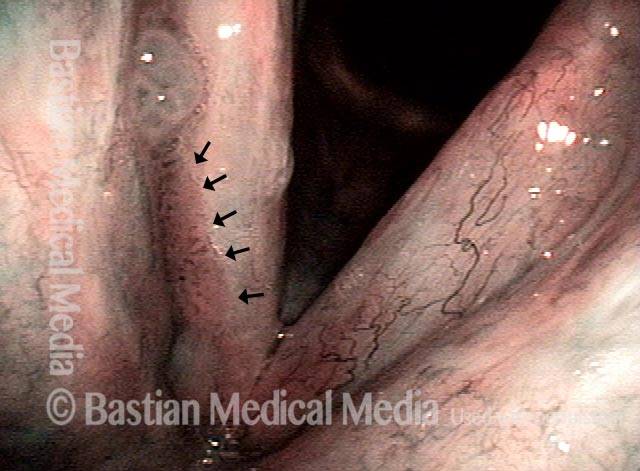
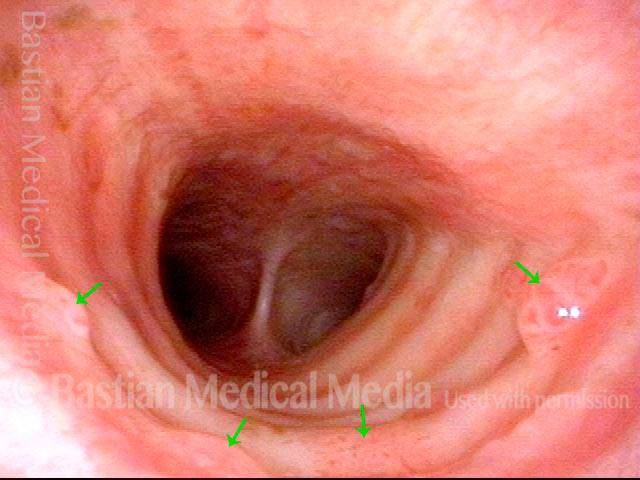
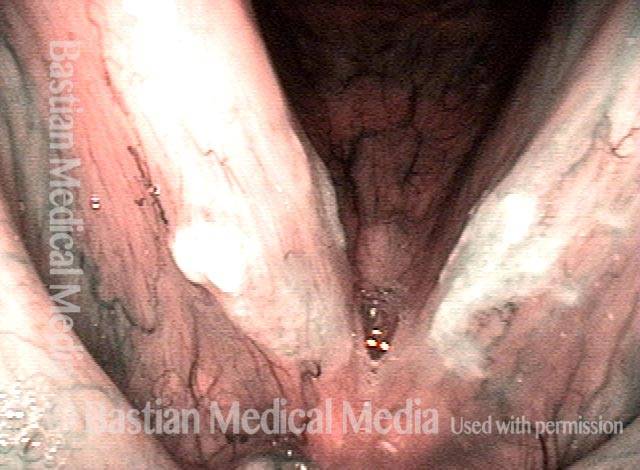
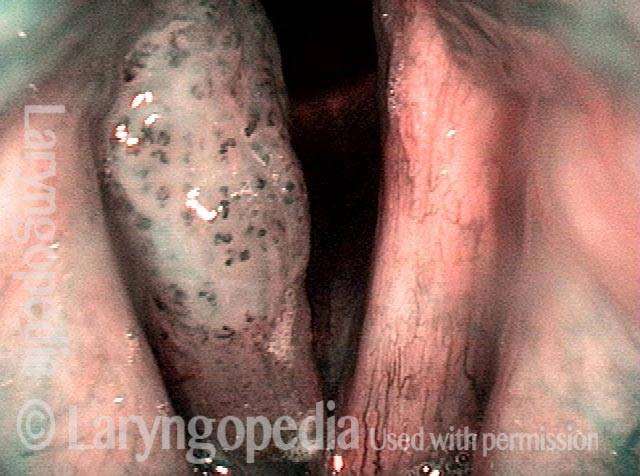
Stippled Vascularity (1 of 8)
HPV infection (2 of 8)
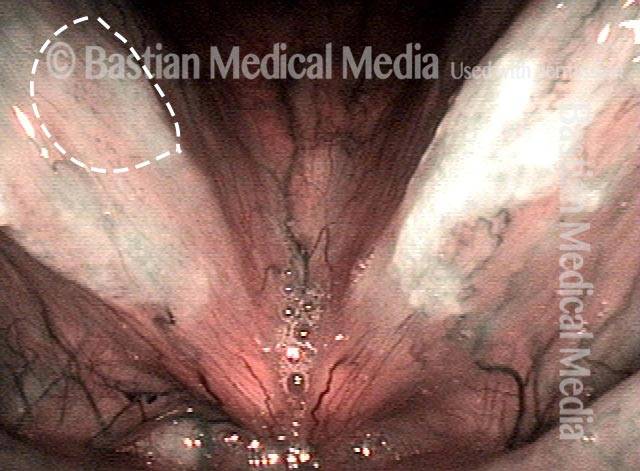
Stippled vascularity (3 of 8)

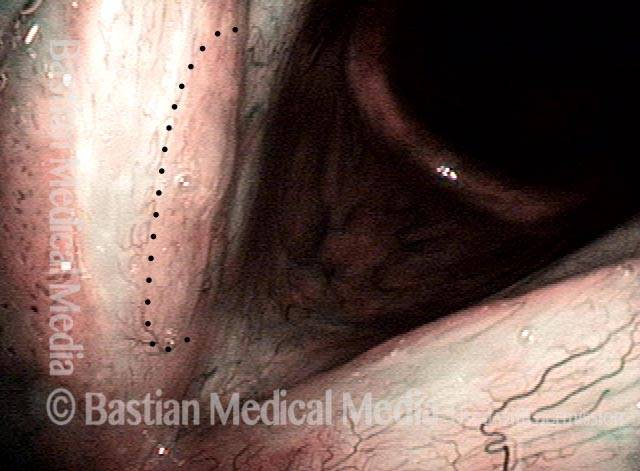
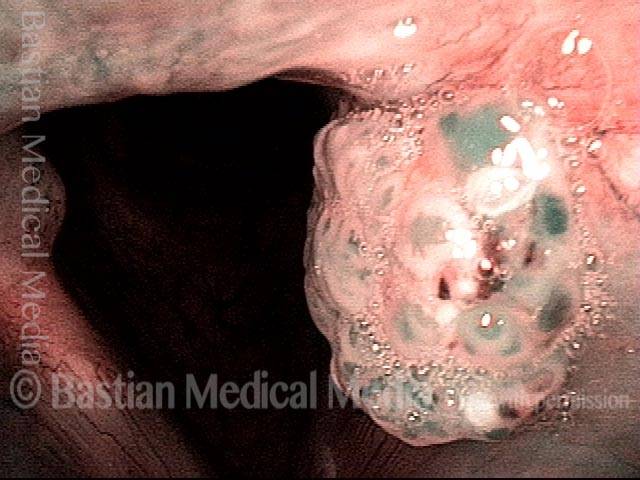
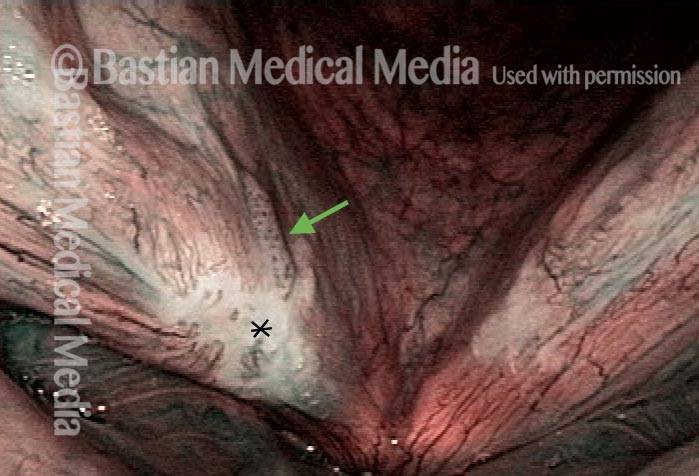
HPV vascular effect (4 of 8)

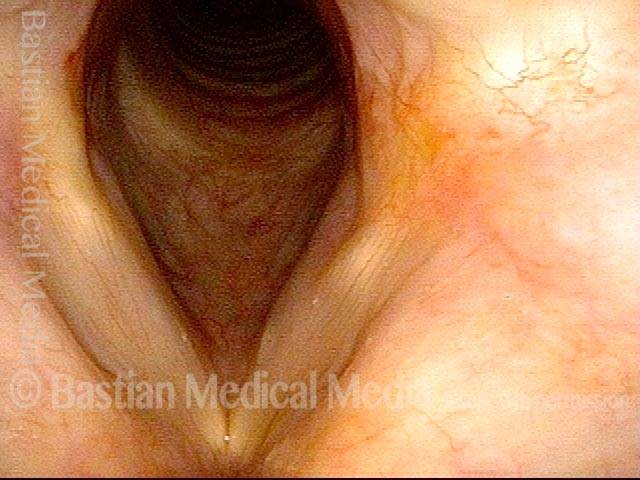
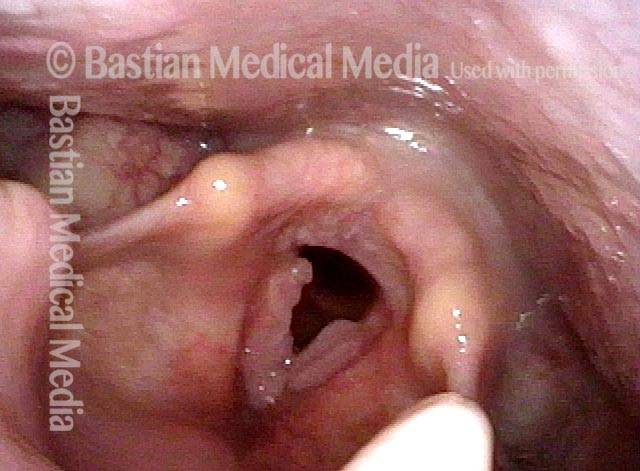
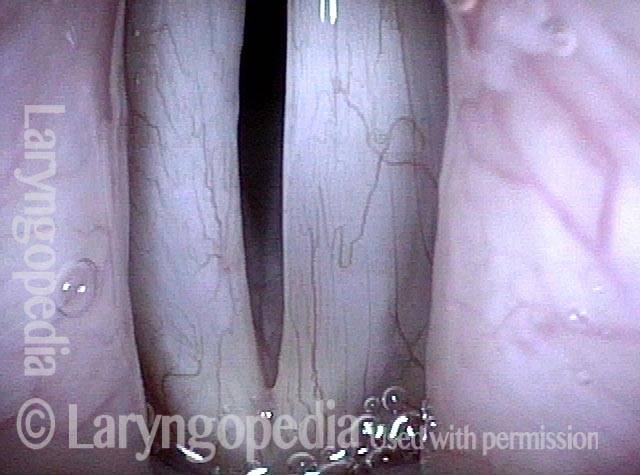
16 months later (5 of 8)
Is it long-term remission? (6 of 8)

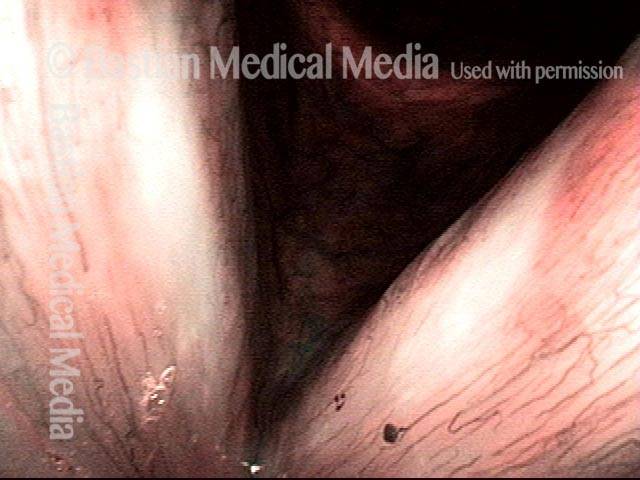
Recurrent Papilloma (7 of 8)
Stippled vascularity (8 of 8)

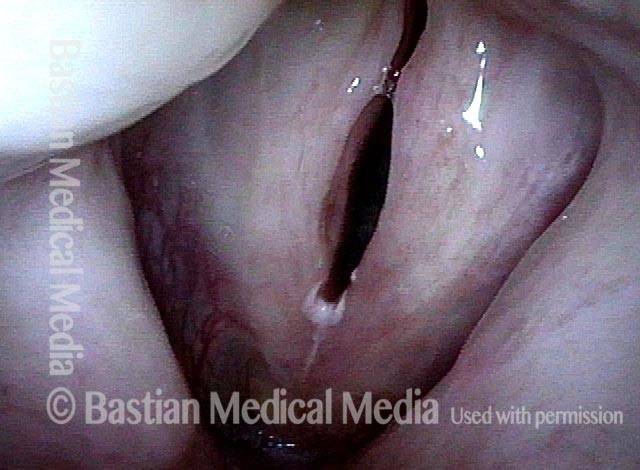
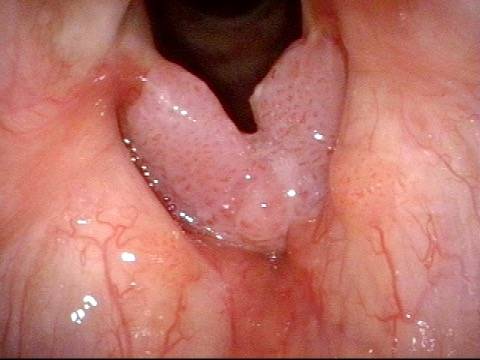
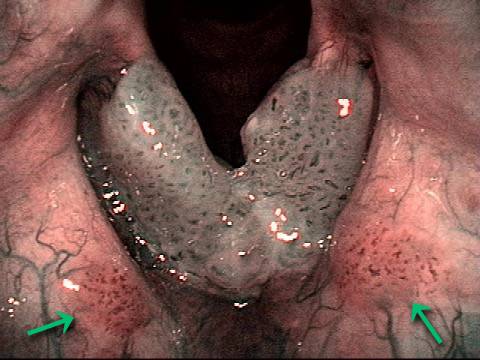
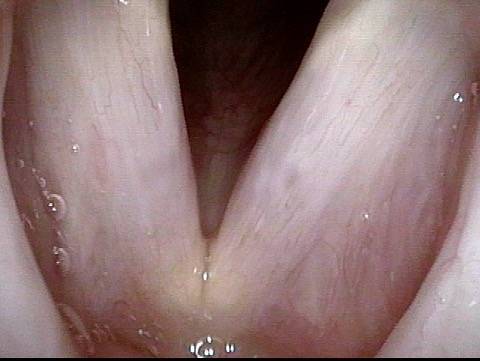
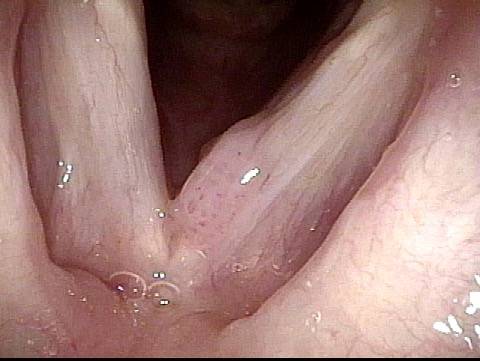
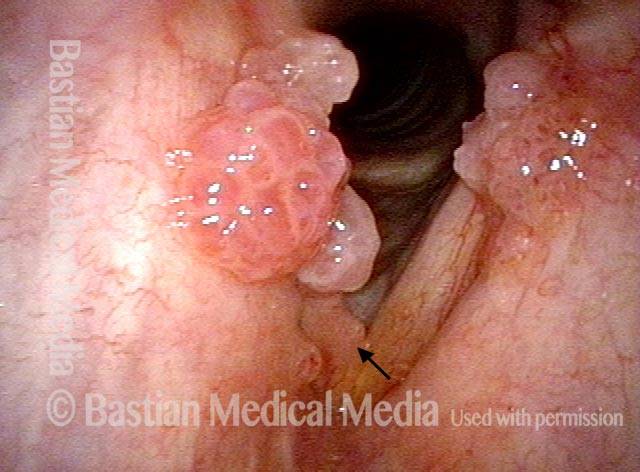
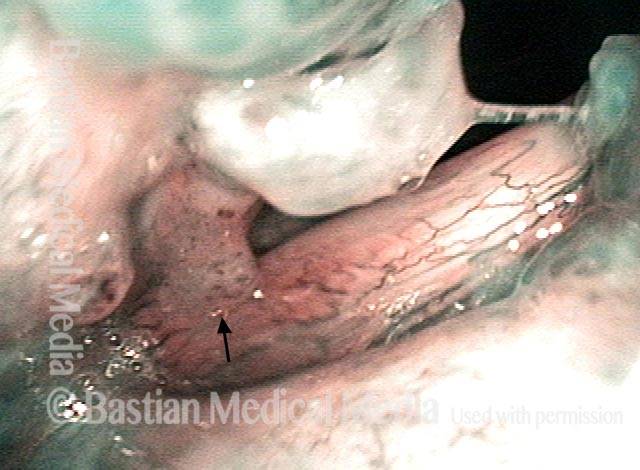
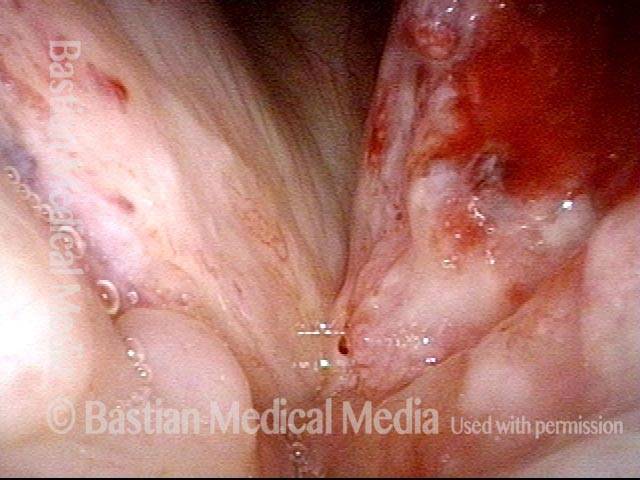
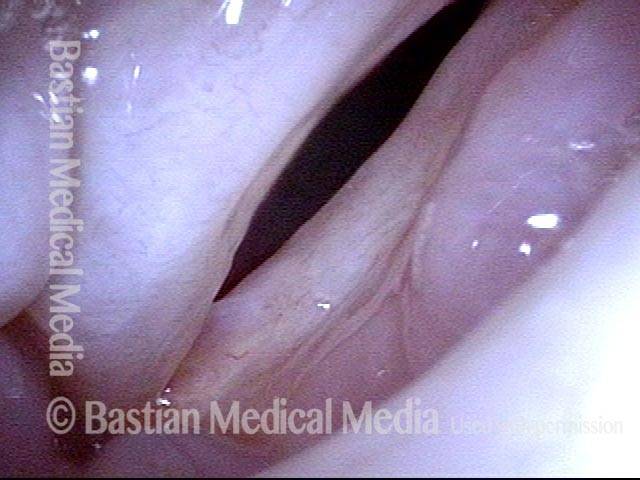
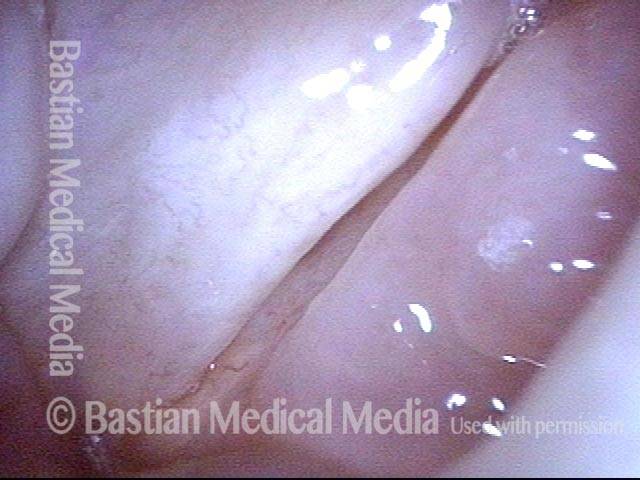
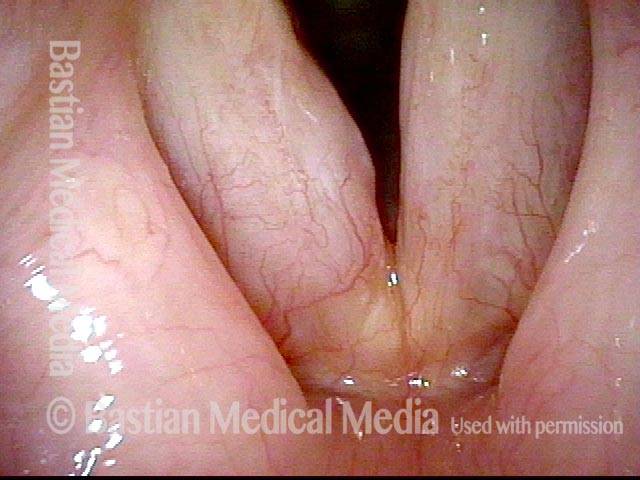
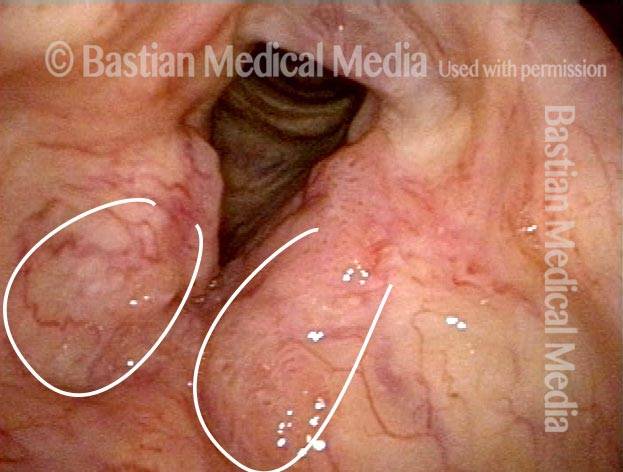
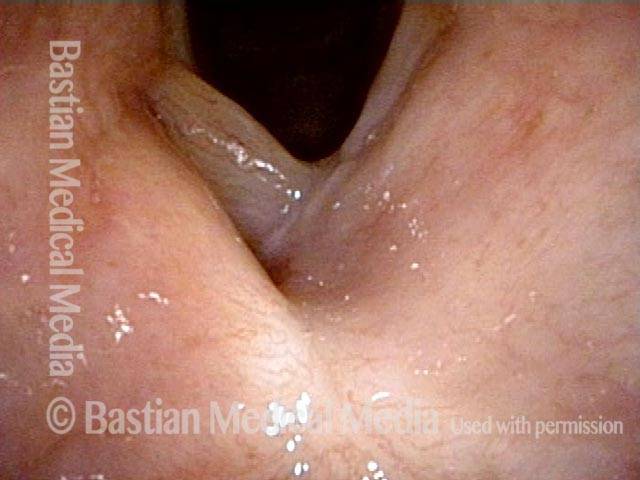
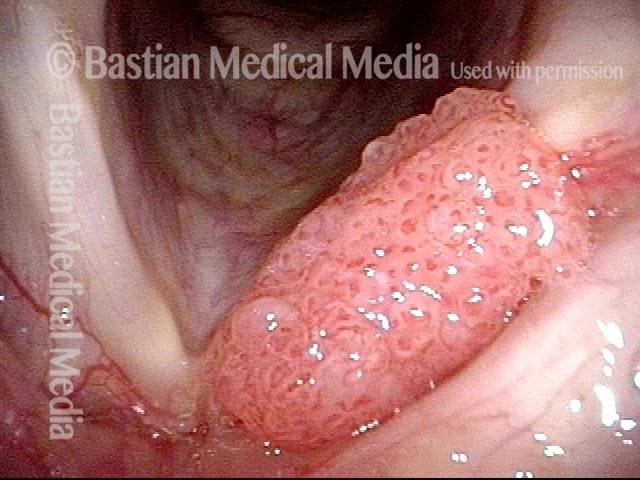
Papillomas, HPV subtype 6, before and after removal
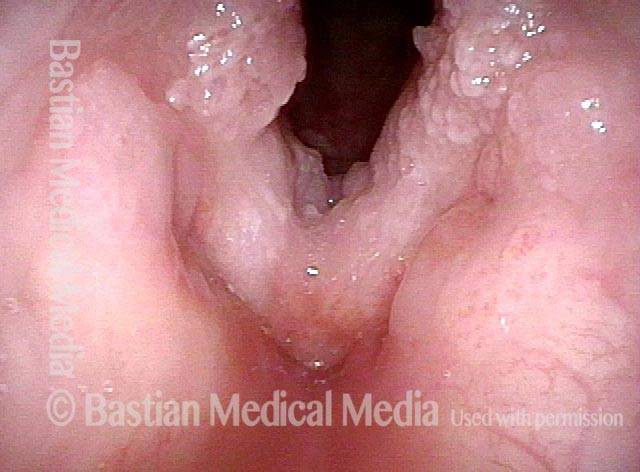
Papillomas: HPV Subtype 6 (1 of 4)

Papillomas: HPV Subtype 6 (2 of 4)

Papillomas, removed: HPV Subtype 6 (3 of 4)

Papillomas, removed: HPV Subtype 6 (4 of 4)
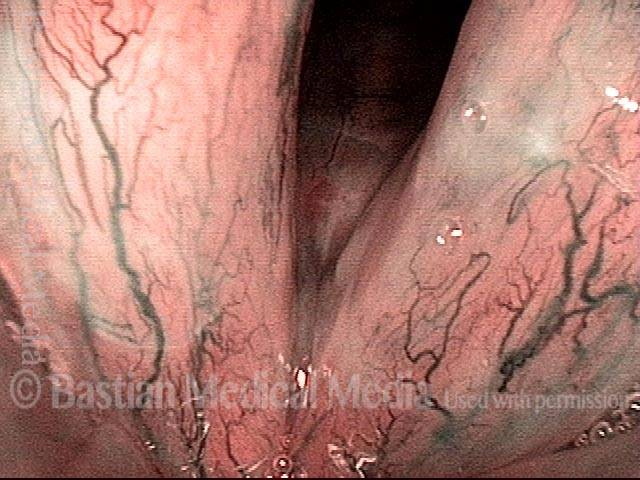
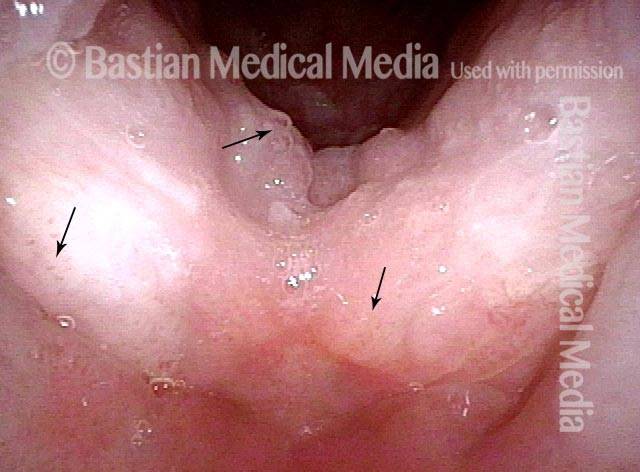
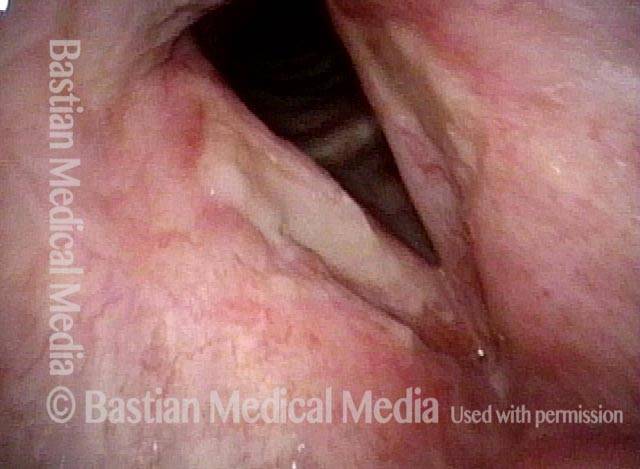
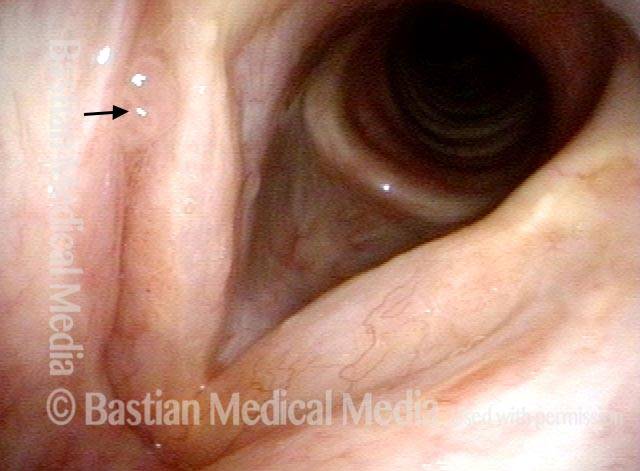
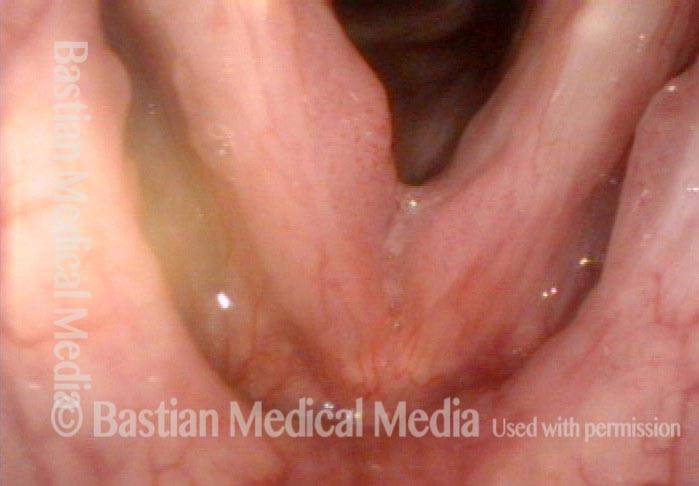
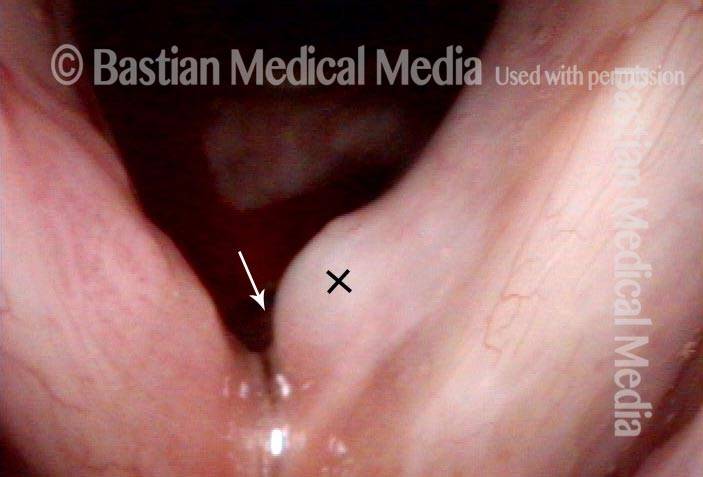
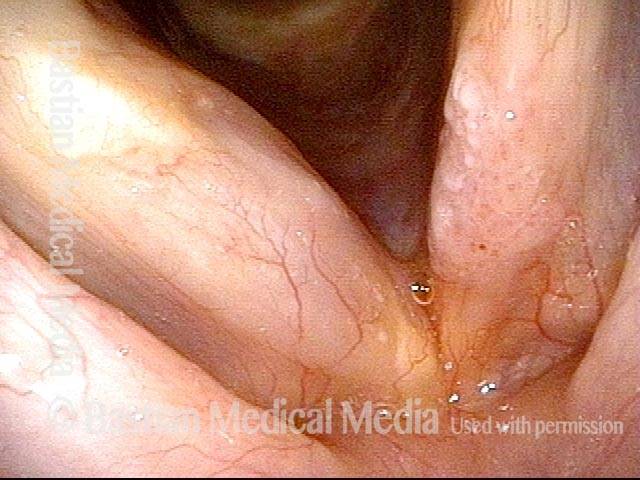
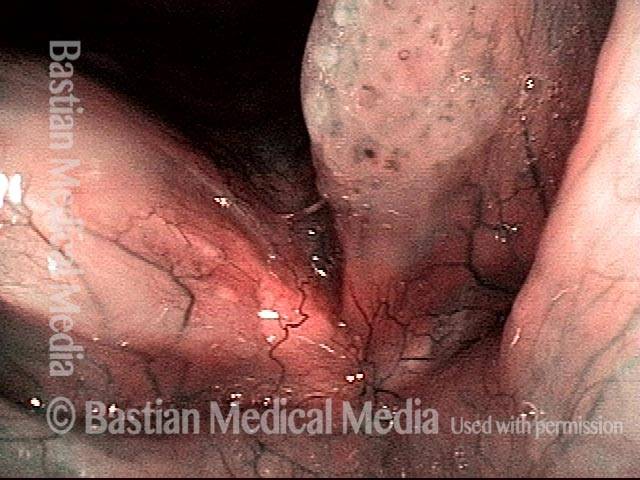
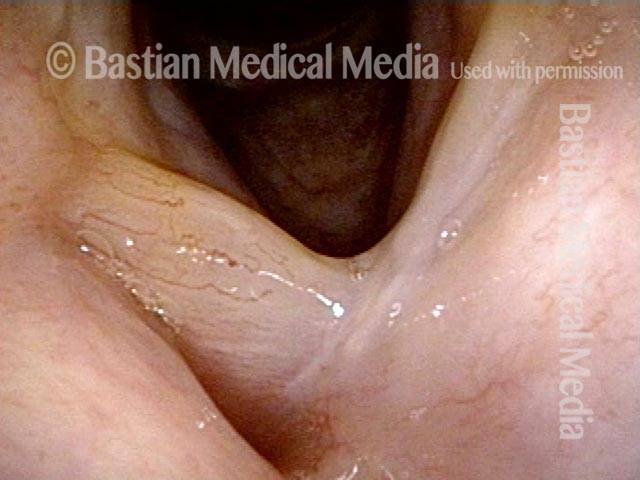
Subtle papillomas, HPV subtype 6
Subtle papillomas, HPV subtype 6 (1 of 3)
Subtle papillomas, HPV subtype 6 (2 of 3)

Subtle papillomas, HPV subtype 6 (3 of 3)
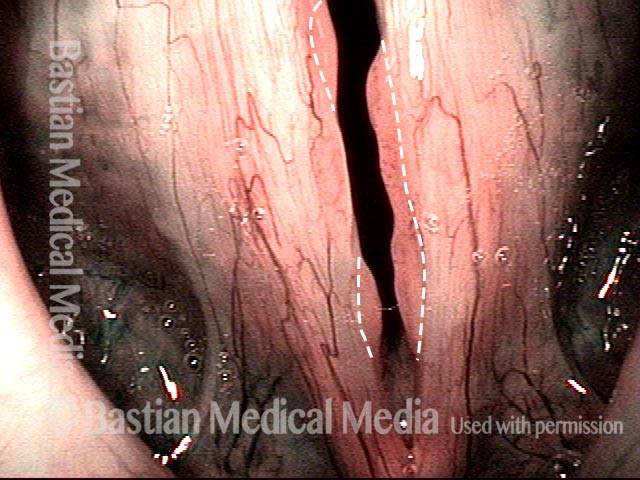
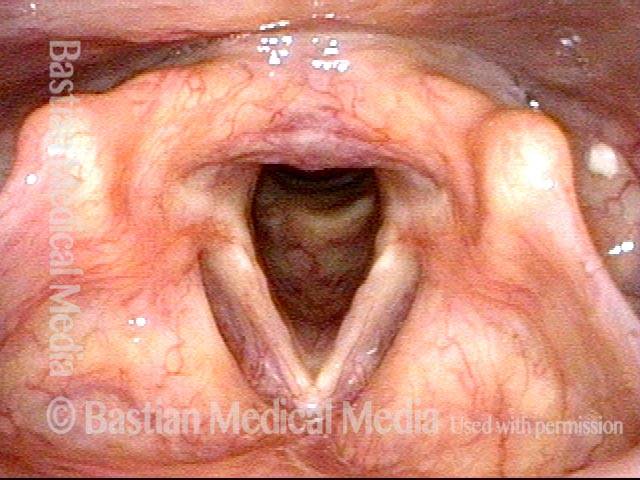
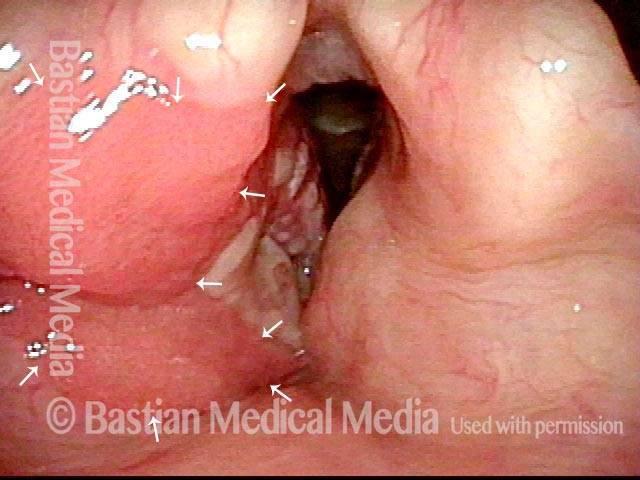
Subtle papillomas and the importance of a motivated examination
Standard light, HPV-6 infection (1 of 4)

Stobe light, vocal cord margin irregularity (2 of 4)
Narrow band light, vascular marks seen (3 of 4)
Narrow band light, papilloma formation (4 of 4)
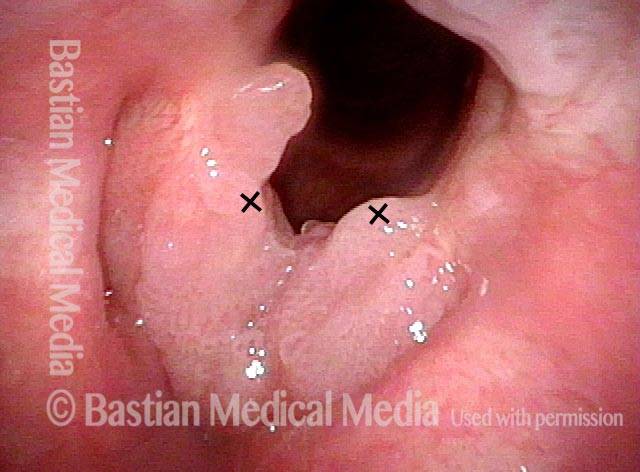
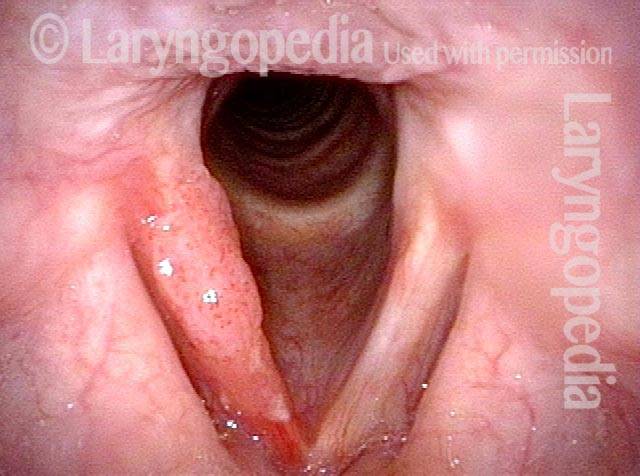
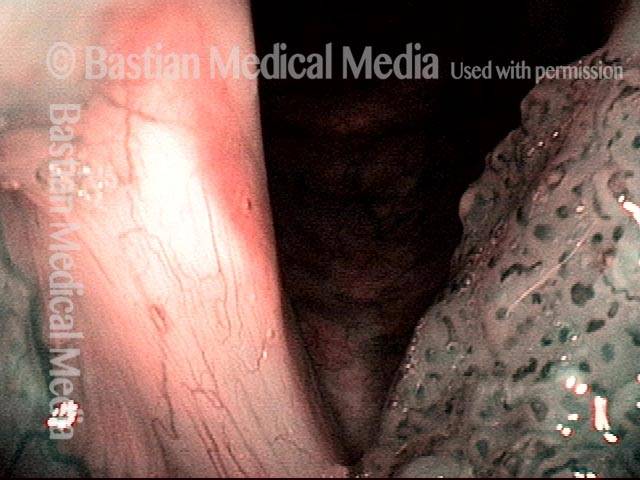
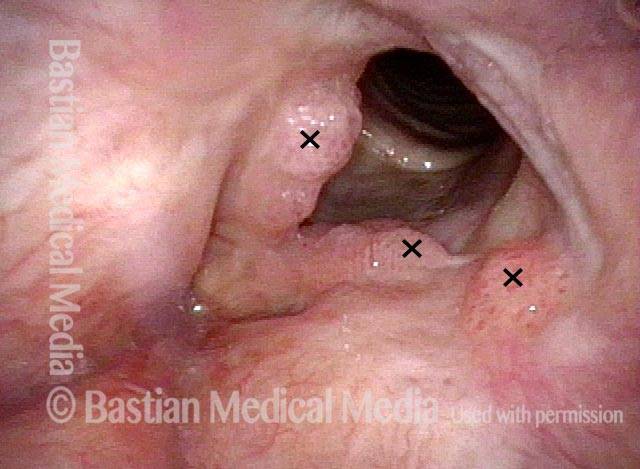
HPV Vascular Effect
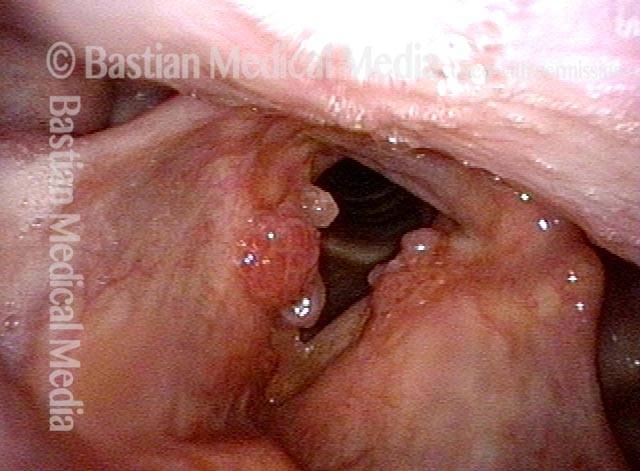
Two papillomas (1 of 3)
Stippled vascularity (2 of 3)

HPV vascular effect (3 of 3)
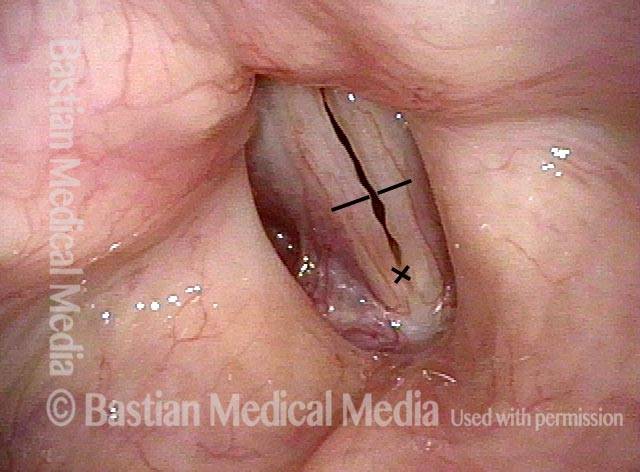
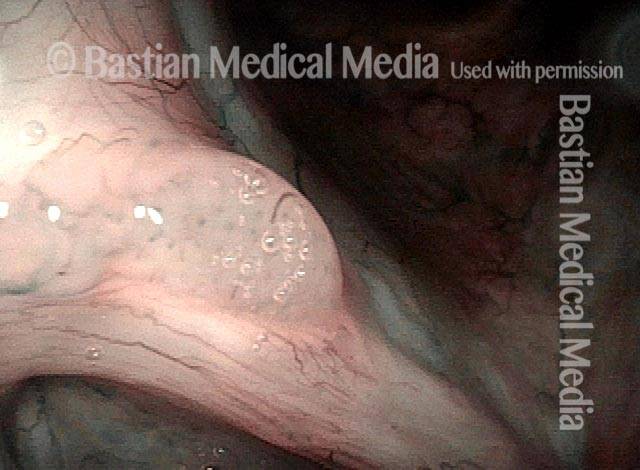
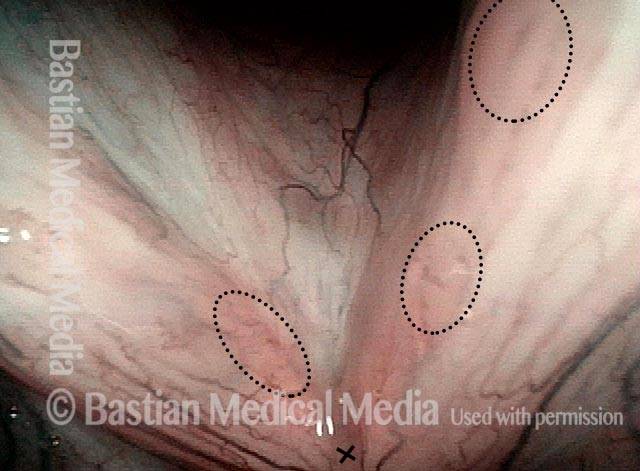
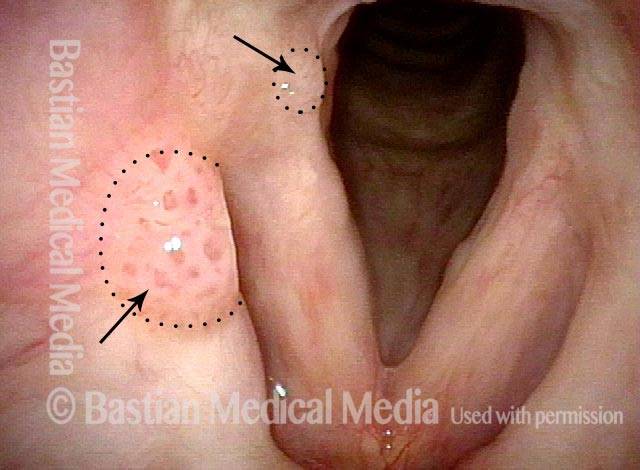
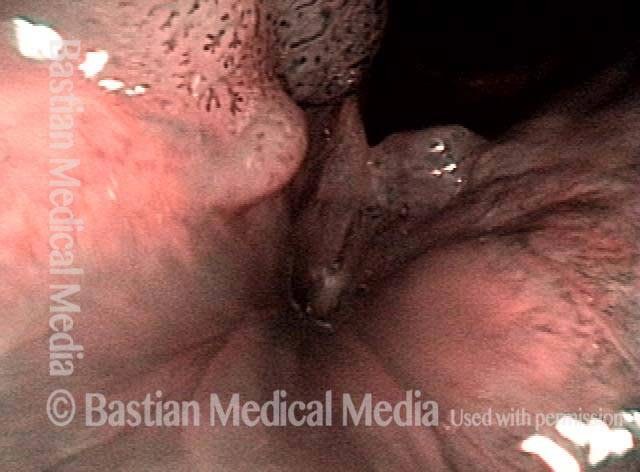
Type 6 HPV Papillomas Firmer Than Most
Stippled vascularity not seen (1 of 4)
HPV vascular effect (2 of 4)
Vascularity clearly seen (3 of 4)

Under narrow-band light (4 of 4)

HPV 6: Going, Going, Gone?
“Curative mode” plan (1 of 7)
Closer view (2 of 7)
Narrow-band illumination (3 of 7)
Post surgery (4 of 7)
Towards “management mode” (5 of 6)
Same view under NBI (6 of 7)
Stippled vascularity seen (7 of 7)
Subtype 11
One of the more common subtypes seen in the airway. HPV 11 is associated with a lesser risk of cancer formation, as well as HPV 6.
Papillomas: HPV Subtype 11 (1 of 3)
Papillomas: HPV Subtype 11 (2 of 3)
Papillomas: HPV Subtype 11 (3 of 3)

Example 2
Papillomas: HPV Subtype 11 (1 of 2)

Papillomas: HPV Subtype 11 (2 of 2)
Papillomas, HPV Subtype 11, Before and After Removal
Papillomas: HPV Subtype 11 (1 of 4)

Papillomas: HPV Subtype 11 (2 of 4)
Papillomas, removed: HPV Subtype 11 (3 of 4)
Papillomas, removed: HPV Subtype 11 (4 of 4)

Subtype 16
Less common in the airway than the more common subtypes 6 and 11. HPV 16 is associated with a higher risk of cancer formation, along with HPV subtypes 18, 31, 45, 55, and others.
Lesions of HPV Subtype 16
Lesions of HPV Subtype 16 (1 of 3)

Lesions of HPV Subtype 16 (2 of 3)

Lesions of HPV Subtype 16 (3 of 3)

Cancer, HPV Subtype 16, Before and After Radiation
Cancer: HPV Subtype 16 (1 of 5)
Cancer: HPV Subtype 16 (2 of 5)
Cancer: HPV Subtype 16, after radiation therapy (3 of 5)

Cancer: HPV Subtype 16, after radiation therapy (4 of 5)
Cancer: HPV Subtype 16, after radiation therapy (5 of 5)
Subtype 18
This is less common in the airway than the more common subtypes 6 and 11. HPV 18 is associated with a higher risk of cancer formation, along with HPV subtypes 16, 31, 45, 55, and others.
Papillomas seen (1 of 4)
Stippled vascularity (2 of 4)

Surgical removal (3 of 4)

Cidofovir injection (4 of 4)
Subtype 31
This is less common in the airway than the more common subtypes 6 and 11. HPV 31 is associated with a higher risk of cancer formation, along with HPV subtypes 16, 18, 45, 55, and others.
Papillomas, HPV Subtype 31, Going Into Remission
Papillomas: HPV Subtype 31 (1 of 4)
Papillomas: HPV Subtype 31 (2 of 4)
Papillomas, in remission: HPV Subtype 31 (3 of 4)
Papillomas, in remission: HPV Subtype 31 (4 of 4)

HPV 31 As A Cause of “Chronic Laryngitis”
Hazy leukoplakia, HPV suspected (1 of 4)

Leukoplakia remains (2 of 4)

Leukoplakia demarcated (3 of 4)
HPV effect confirmed (4 of 4)
HPV 31 → Cancer → Cure
Carcinoma in situ (1 of 4)

HPV subtype 31 (2 of 4)
Excisions (3 of 4)

Seven years later (4 of 4)

Subtype 44
Voiceless 50-year-old man (1 of 6)
Vascular stippling (2 of 6)
Narrow band light, vascularity (3 of 6)

4 months later, recurrent papillomas (4 of 6)
Open position, narrow band light (5 of 6)

Closing for voicing (6 of 6)

Example 2
Stippled vascularity (1 of 4)

Narrow-band lighting (2 of 4)
4 months later (3 of 4)

Closer view (4 of 4)

Subtype 45
This subtype is less common in the airway than the more common subtypes 6 and 11. HPV 45 is associated with a higher risk of cancer formation, along with HPV subtypes 16, 18, 31, 55, and others.
Papillomas: HPV Subtype 45 (1 of 2)
Papillomas: HPV Subtype 45 (2 of 2)

Example 2
HPV type 45 detected (1 of 7)
Closer view of HPV effect (2 of 7)

Narrow band illunination (3 of 7)

Post radiotherapy, glottic web seen (4 of 7)
Post-radiation web (5 of 7)
Post-microlaryngoscopy, release of glottic web (6 of 7)

HPV effect no longer seen (7 of 7)

Subtypes 33 & 45
Hoarse voice (1 of 5)
Narrow band light (2 of 5)
Post excision (3 of 5)

Healed (4 of 5)

“Cured” (5 of 5)
Subtype 55
This subtype is less common in the airway than the more common subtypes 6 and 11. HPV 55 is associated with an intermediate degree of risk of cancer formation, as compared to other subtypes of HPV.
Papillomas, HPV Subtype 55, Going Into Remission
Papillomas: HPV Subtype 55 (1 of 4)

Papillomas: HPV Subtype 55 (2 of 4)

Papillomas, in remission: HPV Subtype 55 (3 of 4)

Papillomas, in remission: HPV Subtype 55 (4 of 4)
Subtype 69
HPV Subtype 69 (High-Intermediate Risk)
Standard lighting (1 of 2)
Narrow band lighting (2 of 2)
HPV 84 & 11
Chronic hoarseness, papilloma (1 of 5)
Stippled vascularity, leukoplakia (2 of 5)

Post treatment, voice is very good (3 of 5)

Closed phase (4 of 5)

Open phase (5 of 5)